|
View the:
Paper (author's version)
Paper (JVIR)
Slides
Scrollable CT of a transgastric pancreatic duct drain
|
Boas FE, Kelly P, and Shlansky-Goldberg R. (2014) "Targeted transgastric drainage of persistent pancreaticocutaneous fistulas." JVIR 25(3): S41. Presented at SIR, San Diego, 2014-03-23.
Boas FE, Kadivar F, Kelly PD, Drebin JA, Vollmer CM, Shlansky-Goldberg RD. (2015) "Targeted transgastric drainage of isolated pancreatic duct segments to cure persistent pancreaticocutaneous fistulas from pancreatitis." J Vasc Interv Radiol. 26(2):247-51.
Abstract
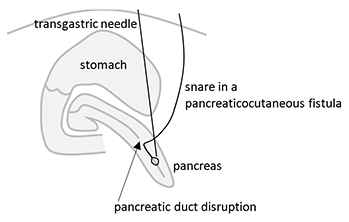
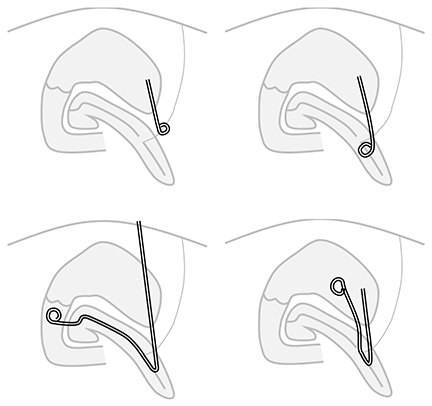
Chronic pancreaticocutaneous fistulas can be difficult to treat. This paper presents a snare-target technique for draining a non-dilated pancreatic duct into the stomach, thus diverting pancreatic fluid away from the pancreaticocutaneous fistula to allow it to heal. Internal or internal/external transgastric pancreatic duct or fistula drains were placed in 6 patients. After an average of 4 months of drainage, all 6 patients had resolution of the cutaneous fistula. 2 patients developed a pseudocyst but no recurrent fistula after drain removal, and the other 4 had no pseudocyst or fistula after an average of 27 months follow up (range 6-74 months).
Keywords: pancreatic fistula, pancreatic duct injury, pseudocyst, transgastric drain, snare
|